You’ve seen the headlines. You probably know someone using it. Maybe you’re using it yourself. Ozempic, Wegovy, Mounjaro, Zepbound… the GLP-1 medications have become the most talked-about weight loss tools in a generation, and for good reason: they work.
But here’s what almost no one is telling you, and it’s the single most important thing you’ll read about these drugs:
The medication doesn’t actually make you lose fat. You do. The medication just finally makes it possible.
That’s not a criticism of these drugs. I do think they’re one of the most remarkable advances in obesity treatment we’ve ever had. It’s a warning. Because if you don’t understand how they work, you’re very likely to be one of the people who regains everything within two years of stopping. And the data on that is sobering.
Let me walk you through exactly what’s happening inside your body and what you need to do to make sure your results actually last.
First, a Quick Reminder: How Fat Loss Works
If you’ve read my article on how fat loss actually works, you already know the foundation. If not, here’s the one-sentence version:
The only way to lose fat is to sustain a caloric deficit over time is consuming less energy than your body burns.
No medication changes this law. Not Ozempic, not Mounjaro, not anything that exists or ever will. Keep that anchored in your mind, because everything below builds on it.
So if the deficit is what causes fat loss, the real question becomes: why is sustaining that deficit so brutally hard for so many people? And that’s exactly the question GLP-1 medications answer.
Your Gut Talks to Your Brain — Constantly
Your body has an extraordinarily sophisticated communication system between your digestive tract and your brain. Much of it is run by hormones called incretins.
When you eat, your intestine releases incretin hormones to prepare your body for the incoming energy. The two most important are GLP-1 (glucagon-like peptide-1) and GIP (gastric inhibitory polypeptide). In a healthy system, the moment food touches your intestinal lining, these hormones fire off and do several things at once:
- They signal your pancreas to release insulin (to manage incoming glucose)
- They suppress glucagon (a hormone that raises blood sugar)
- They slow down how fast your stomach empties
- And, most importantly for weight, they travel to your brain and tell it you’re satisfied
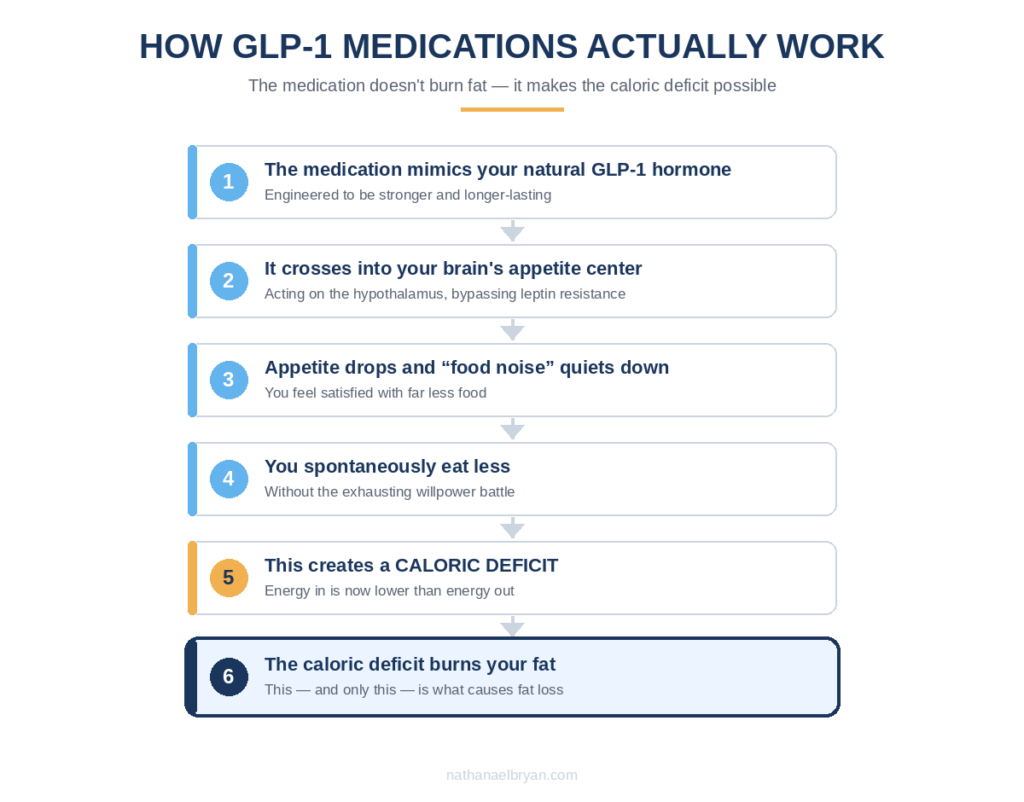
GLP-1 medications are synthetic versions of that natural GLP-1 hormone, engineered to be far more powerful and to last much longer in your body. So they take this normal, healthy appetite-regulation system and turn the volume way up.
The Real Magic Is in Your Brain
Here’s where it gets fascinating and where most explanations stop short.
The most important thing these medications do isn’t in your stomach or your pancreas. It’s in your brain.
Modern GLP-1 medications were specifically designed to cross the blood-brain barrier, a highly selective filter that protects your brain from most substances in your bloodstream. Once across, the medication reaches your hypothalamus, the master control center for appetite. There, it acts directly on the neurons that govern hunger and fullness.
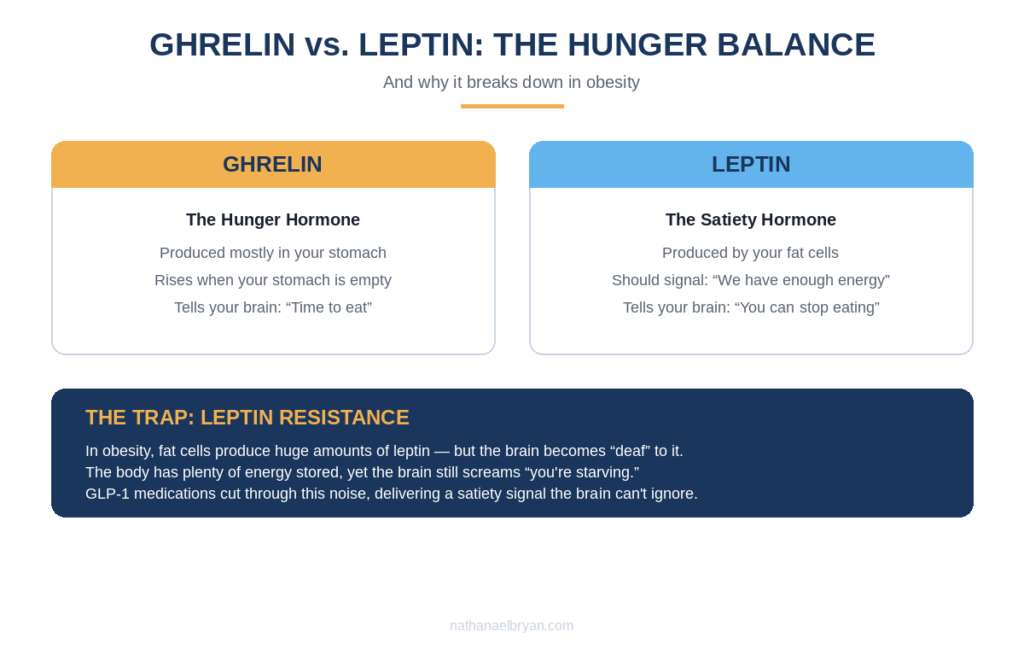
To understand why this matters so much, you need to meet two hormones: ghrelin and leptin.
- Ghrelin is your “hunger hormone.” It’s produced mostly in your stomach, and its levels rise when your stomach is empty, driving you to eat.
- Leptin is your “satiety hormone.” It’s produced by your fat cells and is supposed to tell your brain: “We have plenty of energy stored, you can stop eating now.”
In theory, someone carrying a lot of body fat should have tons of leptin and feel perfectly satisfied. But that’s not what happens. Instead, people with obesity develop something called leptin resistance.
Leptin Resistance: The Cruel Trap of Obesity
This is the part I wish someone had explained to me when I was obese and being told to “just eat less.”
When you have a large amount of body fat, your fat cells produce enormous amounts of leptin. You’d think that would mean constant satiety. But the brain, flooded with this nonstop signal, essentially goes “deaf” to it. It stops hearing the message.
The result is a devastating feedback failure: your body has plenty of energy stored, but your brain still thinks you’re starving. It keeps sending hunger signals. It keeps demanding food. And the person on the receiving end is told they simply lack willpower.
This is not a character flaw. It’s a broken biological signal. And it’s exactly why “just eat less” fails so reliably for people with obesity: they’re being asked to consciously override a survival system that’s screaming at them all day long.
Here’s where GLP-1 medications change everything. They provide a satiety signal so strong and so direct that it bypasses the leptin resistance entirely. They quiet the relentless “food noise” (that constant mental chatter about food that dominates so many people’s minds) and hand back control over eating decisions.
For the first time, often in years, the person feels normal around food. Not deprived. Not obsessed. Just… satisfied with less.
So Here’s What Actually Happens
Now we can put the whole picture together. When someone takes a GLP-1 medication:
- Their appetite drops dramatically
- The food noise quiets down
- Their stomach empties more slowly, so they feel full longer
- They spontaneously eat less, without the agonizing willpower battle
- This creates a caloric deficit
- The caloric deficit burns their fat
Read that sequence again, because it contains the entire truth about these medications:
The drug didn’t burn the fat. The deficit did. The drug just made the deficit achievable.
The medication removed the herculean suffering of fighting against a biology designed to hoard energy. That’s an enormous, genuinely valuable thing. But it’s a fundamentally different claim than “the medication melts fat.”
The Contradiction That Reveals Everything
You’ve probably heard someone say and maybe you’ve said it yourself:
“I dieted for years and never lost weight. But the moment I started Mounjaro, the weight finally came off!”
Now that you understand the mechanism, you can see the logical error hiding in that sentence.
If you weren’t losing fat before, it’s because you weren’t actually in a caloric deficit, no matter how carefully you believed you were dieting. You were eating at or above your maintenance level, likely because your biology made true hunger impossible to ignore.
The medication didn’t rewrite the laws of physics. It reduced your appetite so profoundly that you began eating less and finally achieved the very deficit that had eluded you. The fat loss came from the same caloric deficit you were chasing all along. The drug just made it possible to sustain.
This isn’t pedantry. Understanding this distinction is the difference between keeping your results and losing them.
Why So Many People Regain Everything
Here’s the statistic that should give every GLP-1 user pause: studies show that the majority of people regain most of the weight they lost within one to two years of stopping the medication.
Why? Now you have the tools to understand it completely.
The medication was doing the heavy lifting: suppressing appetite, quieting food noise, making the deficit feel effortless. But if that’s all that happened, then nothing actually changed about the person’s life:
- They never learned how to eat for their body
- They never built sustainable habits
- They never developed a healthy relationship with food
- They never addressed the behaviors that led to weight gain in the first place
So when the medication stops, the appetite roars back. The food noise returns. The old patterns are still there, waiting. And the fat cells (which never disappeared, they only shrank) are ready to refill.
The medication was a bridge. But if you don’t use the time on that bridge to build something permanent on the other side, you just walk right back to where you started.
The Side Effect Nobody Talks About: Muscle Loss
There’s a critical danger with GLP-1 medications that gets far too little attention, and it’s the one I worry about most as a nutritionist.
When you lose weight rapidly while eating much less food, a significant portion of what you lose can be muscle, not just fat. Research suggests that without proper nutritional support, 25–40% of the weight lost on GLP-1 medications can be lean mass.
This is a serious problem for several reasons:
- Muscle is metabolically active: losing it lowers your metabolism, making future fat loss harder and regain easier
- Muscle loss accelerates aging, weakens you, and worsens body composition even as the scale drops
- The lower appetite that makes these drugs effective also makes it dangerously easy to under-eat protein (the one nutrient that protects muscle.)

This is precisely why GLP-1 medications should never be used in isolation. Eating less is not the same as eating well. And losing weight is not the same as losing fat.
What Responsible GLP-1 Use Actually Looks Like
If you’re using or considering these medications, here’s what the science says you need alongside them to protect your health and keep your results:
Prioritize protein above everything. This is non-negotiable. Adequate protein (generally 1.6–2.4g per kg of body weight, adjusted to your situation) is what preserves your muscle while you lose fat. With a suppressed appetite, you’ll need to be intentional about hitting it.
Do resistance training. Lifting weights signals your body to keep its muscle during a deficit. Combined with adequate protein, it’s the single best defense against the muscle-loss problem.
Watch your micronutrients. Eating much less food means consuming fewer vitamins and minerals. Deficiencies in B12, iron, calcium, vitamin D, and others become real risks that need monitoring.
Build the behavioral foundation. Use the time on the medication (while food noise is quiet and appetite is manageable) to learn how to eat, build habits, and change your relationship with food. This is the bridge-building that determines whether your results survive after you stop.
Have a plan to stop. These medications aren’t necessarily forever. The discontinuation should be gradual and planned, with nutritional support, not abrupt. (I’ll cover exactly how to do this in a future article.)
Who Should Actually Use These Medications
GLP-1 medications are powerful medical tools, not cosmetic shortcuts. The established clinical criteria exist for good reason:
- Obesity (BMI ≥ 30), or
- Overweight (BMI ≥ 27) with weight-related health conditions like type 2 diabetes, high blood pressure, or sleep apnea
They are not designed for someone who wants to drop 10 pounds for a wedding. Using them casually, without medical supervision and without addressing the nutritional and behavioral foundation, is both medically irresponsible and, as you now understand, a near-guarantee of regain.
The decision to use them is a medical one, made with a physician. My role, and the role of any good nutritionist, is to make sure that if you use them, you do it in a way that protects your muscle, your health, and your long-term results.
The Bottom Line
GLP-1 medications are genuinely revolutionary. They correct a broken biological signal that has caused immeasurable suffering and self-blame for people with obesity. They make the impossible feel possible. I have nothing but respect for what they’ve done for obesity treatment.
But they are a tool, not a cure. They create the conditions for fat loss, they don’t replace the work that makes fat loss last. The deficit still does the work. Your muscle still needs protein and training to survive. Your habits still need to change. And your relationship with food still needs healing.
Use the medication as a bridge. But build something permanent while you’re on it. That’s the difference between a temporary transformation and a permanent one.
Frequently Asked Questions
Does Ozempic burn fat directly?
No. Ozempic (and other GLP-1 medications) reduce your appetite, which leads you to eat less and create a caloric deficit. That deficit is what burns fat. The medication makes the deficit achievable, it doesn’t burn fat on its own.
Will I regain the weight when I stop taking it?
The data shows most people regain the majority of lost weight within 1–2 years of stopping if they didn’t build sustainable habits and nutritional knowledge while on the medication. The regain isn’t inevitable, but avoiding it requires using your time on the drug to change your eating patterns, preserve muscle, and develop food autonomy.
Why am I losing muscle on Ozempic?
Rapid weight loss combined with a suppressed appetite often means inadequate protein intake, which causes your body to break down muscle alongside fat. Studies suggest 25–40% of weight lost on GLP-1 medications can be lean mass without proper nutrition and resistance training. Prioritizing protein and lifting weights is essential.
How much protein do I need on a GLP-1 medication?
Generally 1.6–2.4g per kg of body weight, adjusted to your individual situation. Because these medications suppress appetite, you’ll need to be deliberate about hitting your protein target; it won’t happen by accident.
Are GLP-1 medications safe?
For appropriate candidates under medical supervision, they have a well-studied safety profile, though they carry side effects (nausea, GI issues, and rarer risks like pancreatitis). They should only be used under the guidance of a physician, with clinical criteria met. The nutritional risks (muscle loss and nutrient deficiencies) are manageable with proper support.
Can I take Ozempic just to lose a few pounds?
These medications are designed for treating obesity (BMI ≥ 30) or overweight (BMI ≥ 27) with related health conditions, not for cosmetic weight loss. Casual use without medical supervision is both irresponsible and likely to result in regain once stopped.